HEALTH & NUTRITION
As with most of the other information I have shared it would be nearly impossible to say everything I learned. Moreover, I have chosen not to write about HIV/AIDS or other specific illnesses. My goal is to provide a general overview. As such, I will simply summarize a few things that stuck out to me during my tours of several hospitals, clinics and also during lectures. Information from our student handbook and also a lecture entitled: "Health Systems, The Ugandan Health System" delivered during our course in Madison has also be included. Please feel free to follow-up for more information.
Ministry of Health

Uganda’s Ministry of Health works to establish national health policies, guidelines and standards as well as to ensure good health for all people in Uganda. The Ministry manages nationally based health services, conducts research in health-related fields, develops health infrastructure, and ensures sufficient training of health care professionals.
More information may be found here: http://www.health.go.ug/
More information may be found here: http://www.health.go.ug/
Traditional Healers
These include spiritualists (ex: Hot Springs), herbalists (ex: Wandegya lab), bone Setters and traditional birth attendants. These individuals play an important role in the health care dissemination in Uganda. Many people trust these people and believe in their skils over physicians. Those who believe in traditional healers typically visit them before they seek care in the hospital setting. We had an opportunity to share with a traditional birth attendant. she had been practicing for over 30 years and birthed babies in a home environment. She has received some training from the government and was certain to always refer difficult cases to the hospital setting. Pictures/video of this visit below.
Notes about Traditional Healers:
- First line of healing
- Accessible
- Culturally appropriate
- Affordable
- Efficacy uncertain
- Regulations, certification and standards vary
Notes about Traditional Healers:
- First line of healing
- Accessible
- Culturally appropriate
- Affordable
- Efficacy uncertain
- Regulations, certification and standards vary








Allopathic (Western) Medicine
Government: free
Uganda National Minimum Health Care Package Clusters
- Health promotion, community health
- Maternal and child health
- Communicable diseases
- Non-communicable diseases
- Per capita expenditure on health: 12 US Dollars (World Health
Organization, WHO recommends $35 as such healthcare is not
universally accessible.
Private: cost varies
- Referral hospital= 5,000 shillings per visit (2.50 US dollars)
- Village hospital= 2,000 shillings per vists (1 US dollar)
Mission based: religiously funded
Notes about Allopathic (Western) Medicine:
- Scarce resources
- Facilities often inaccessible and/or overcrowded and understaffed
- Not user friendly
- Expensive
- Regulations and standards variably enforced
Uganda National Minimum Health Care Package Clusters
- Health promotion, community health
- Maternal and child health
- Communicable diseases
- Non-communicable diseases
- Per capita expenditure on health: 12 US Dollars (World Health
Organization, WHO recommends $35 as such healthcare is not
universally accessible.
Private: cost varies
- Referral hospital= 5,000 shillings per visit (2.50 US dollars)
- Village hospital= 2,000 shillings per vists (1 US dollar)
Mission based: religiously funded
Notes about Allopathic (Western) Medicine:
- Scarce resources
- Facilities often inaccessible and/or overcrowded and understaffed
- Not user friendly
- Expensive
- Regulations and standards variably enforced
Government Health System
(Listed as: levels, number, pop served)
National Referral Hospital
1: 27 million (Mulago)
Regional Referral Hospitals
12: 2 million (Govt + mission)
District Health Services and Health Centers
Level I: 1,000 (village)
Level II: 5,000 (parish)
Level III: 20,000 (subcounty)
Level IV: 100-500,000 (district)
National Referral Hospital
1: 27 million (Mulago)
Regional Referral Hospitals
12: 2 million (Govt + mission)
District Health Services and Health Centers
Level I: 1,000 (village)
Level II: 5,000 (parish)
Level III: 20,000 (subcounty)
Level IV: 100-500,000 (district)
Village Health Team
Health Center Level I
- Village health teams-up to 10 people
- At least 1/3 women
- Coordinated by Village Local Councils
- Assess needs
- Mobilize resources
- Select and monitor community health workers
- Maintain household registry-census
- First level of formal health care
Health Center II
- Ambulatory care
- Staffed by comprehensive nurses
- Immunizations
- Health education
- Linked to village health team
Health Center Level III
- Preventive services
- Supervision of level I and II services
- Laboratory
- Maternity care
- Referral to Level IV
Health Center Level IV
- Preventive, curative, rehabilitative
- Medical, surgical and obstetrical car
- Base for supervision of HC I, II and III services
- Data collection and assimilation
Mission Hospitals and Clinics
- 40% of district hospitals
- Variety of local and expatriate staff
- Variety of services
- Government attempting to coordinate services through public-private, not for profit partnerships
District Health
- Services and Responsibilities
- Decentralization into districts (80+) and subdistricts
- Clearly delineated populations
- Service delivery
- Administrative, human and financial management
- Data collection
- Planning and budgeting
- Village health teams-up to 10 people
- At least 1/3 women
- Coordinated by Village Local Councils
- Assess needs
- Mobilize resources
- Select and monitor community health workers
- Maintain household registry-census
- First level of formal health care
Health Center II
- Ambulatory care
- Staffed by comprehensive nurses
- Immunizations
- Health education
- Linked to village health team
Health Center Level III
- Preventive services
- Supervision of level I and II services
- Laboratory
- Maternity care
- Referral to Level IV
Health Center Level IV
- Preventive, curative, rehabilitative
- Medical, surgical and obstetrical car
- Base for supervision of HC I, II and III services
- Data collection and assimilation
Mission Hospitals and Clinics
- 40% of district hospitals
- Variety of local and expatriate staff
- Variety of services
- Government attempting to coordinate services through public-private, not for profit partnerships
District Health
- Services and Responsibilities
- Decentralization into districts (80+) and subdistricts
- Clearly delineated populations
- Service delivery
- Administrative, human and financial management
- Data collection
- Planning and budgeting
Health Indicators
Demographic Indicators
The chart below shows the comparison of Uganda, US and Sweden across several indicators.
Notes:
Total Population
Uganda has a very high population for its area.
Growth Rate
Uganda has the 3rd highest growth rate in the world.
Sweden was chosen to compare because Scandinavian countries tend to be small and stable (good demographics, social and health indicators).
A growth rate of a country is important to understand how they will be able to care for their people. Typically a small growth rate allows the government to plan ahead in order to provide the proper health, education, social, food/water resources its people need. In Uganda's case such a high growth rate makes it difficult to plan.
Total Fertility Rate
In Uganda women have on average 7 children each!
% Under 15
51% of Uganda's population is under the age of 15 which means it is a very dependent population. This structure is primarily due to higher levels of childbearing.
The chart below shows the comparison of Uganda, US and Sweden across several indicators.
Notes:
Total Population
Uganda has a very high population for its area.
Growth Rate
Uganda has the 3rd highest growth rate in the world.
Sweden was chosen to compare because Scandinavian countries tend to be small and stable (good demographics, social and health indicators).
A growth rate of a country is important to understand how they will be able to care for their people. Typically a small growth rate allows the government to plan ahead in order to provide the proper health, education, social, food/water resources its people need. In Uganda's case such a high growth rate makes it difficult to plan.
Total Fertility Rate
In Uganda women have on average 7 children each!
% Under 15
51% of Uganda's population is under the age of 15 which means it is a very dependent population. This structure is primarily due to higher levels of childbearing.
|
|
Socioeconomic Indicators
Notes:
GNI=Gross National Income
PPP= Purchasing Power Parity
Literacy rates for US and Sweden were not included however, they are close to 100% for both.
|
|
Social Status Indicators -- Uganda
- Only 9% of households use electricity for lighting (lanterns are common)
- 68% have access to safe water (tap water, borehole, protected well or spring)
The water must still be prepared properly for sanitation
- 13% have no toilet facilities
- 63% have radios and 6% have television (compared to 99% in the US)
Health Indicators -- Mortality
Notes:
Crude Death Rate is raw/overall #
Infant Mortality is defined as death before first birthday
Indicator
Crude Death Rate
Infant Mortality Under 5 Mortality Rate Maternal Mortality Ratio Physician to population ratio |
|
Causes of Mortality
|
US (1990)
Respiratory Infections
Tuberculosis Gastrointestinal Infections Other infectious diseases US (2000)
Accidents
Homocides Suicide Other chronic diseases (heart, cancer, diabetes) |
Malnutrition
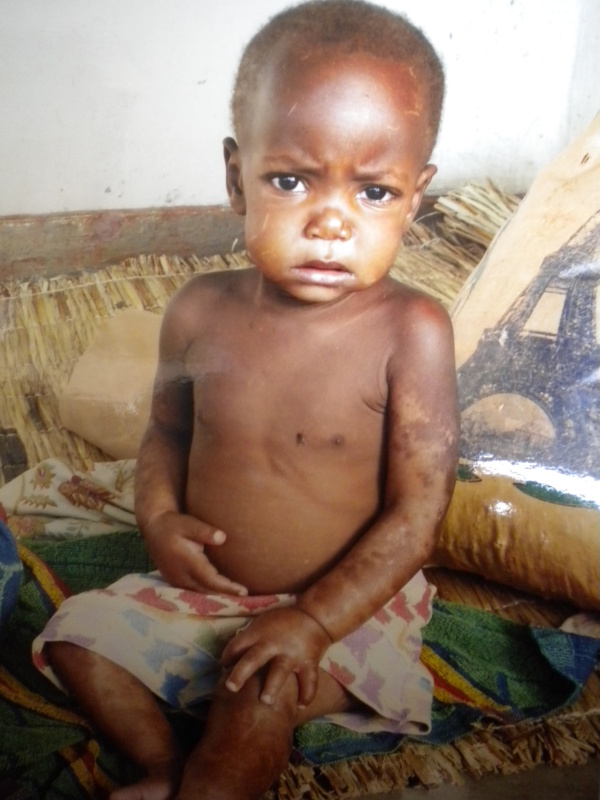
Protein-energy malnutrition is the most severe form of malnutrition in Uganda. There are two types of protein-energy malnutrition: kwashiorkor and marasmus.
Kwashiorkor results from a severe lack of protein in the diet, although overall caloric intake is moderate to good. Kwashiorkor is a common result of diets based on cassava or bananas, foods high in calories but very low in protein. Marasmus is a consequence of a diet severely lacking both protein and calories. A child with kwashiorkor appears bloated while a child with marasmus has a skin-and-bones appearance.
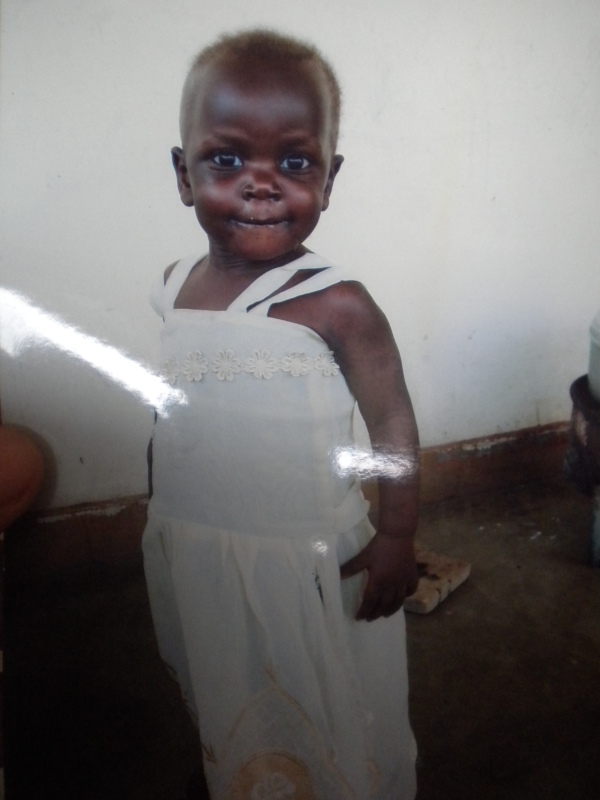
Below you will find before and after photos of a female child who suffered from malnutrition, she is now a healthy and lively little one!
Kwashiorkor results from a severe lack of protein in the diet, although overall caloric intake is moderate to good. Kwashiorkor is a common result of diets based on cassava or bananas, foods high in calories but very low in protein. Marasmus is a consequence of a diet severely lacking both protein and calories. A child with kwashiorkor appears bloated while a child with marasmus has a skin-and-bones appearance.
Below you will find before and after photos of a female child who suffered from malnutrition, she is now a healthy and lively little one!